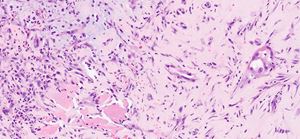
The lesional cells in the case were positive for keratin and PAX8, with negative staining for GATA3, NKX3.1, or p63. The background amyloid-like foci (often seen in this diagnosis) were negative for amyloid by Congo red stain. The correct diagnosis is fibromyxoid nephrogenic adenoma, a rare but reported morphologic pattern of nephrogenic adenoma. On H&E, the most useful feature is searching for classic tubular pattern nephrogenic adenoma, usually present (but can be focal) among the spindle cells and myxoinflammatory background. There should be minimal atypia and/or mitosis. Interestingly, in the largest series of fibromyxoid nephrogenic adenomas, most of the cases occurred in a post-treatment setting of prostate cancer. As such, the key diagnostic pitfall is treated prostatic adenocarcinoma, although sarcomatoid urothelial carcinoma is also in the differential. Immunohistochemically, this variant stains like other nephrogenic adenoma patterns, being positive for PAX8 and negative for NKX3.1. As a cautionary reminder, GATA3, AMACR, PSAP, and PSA can be positive in nephrogenic adenoma.