CASE OF THE WEEK
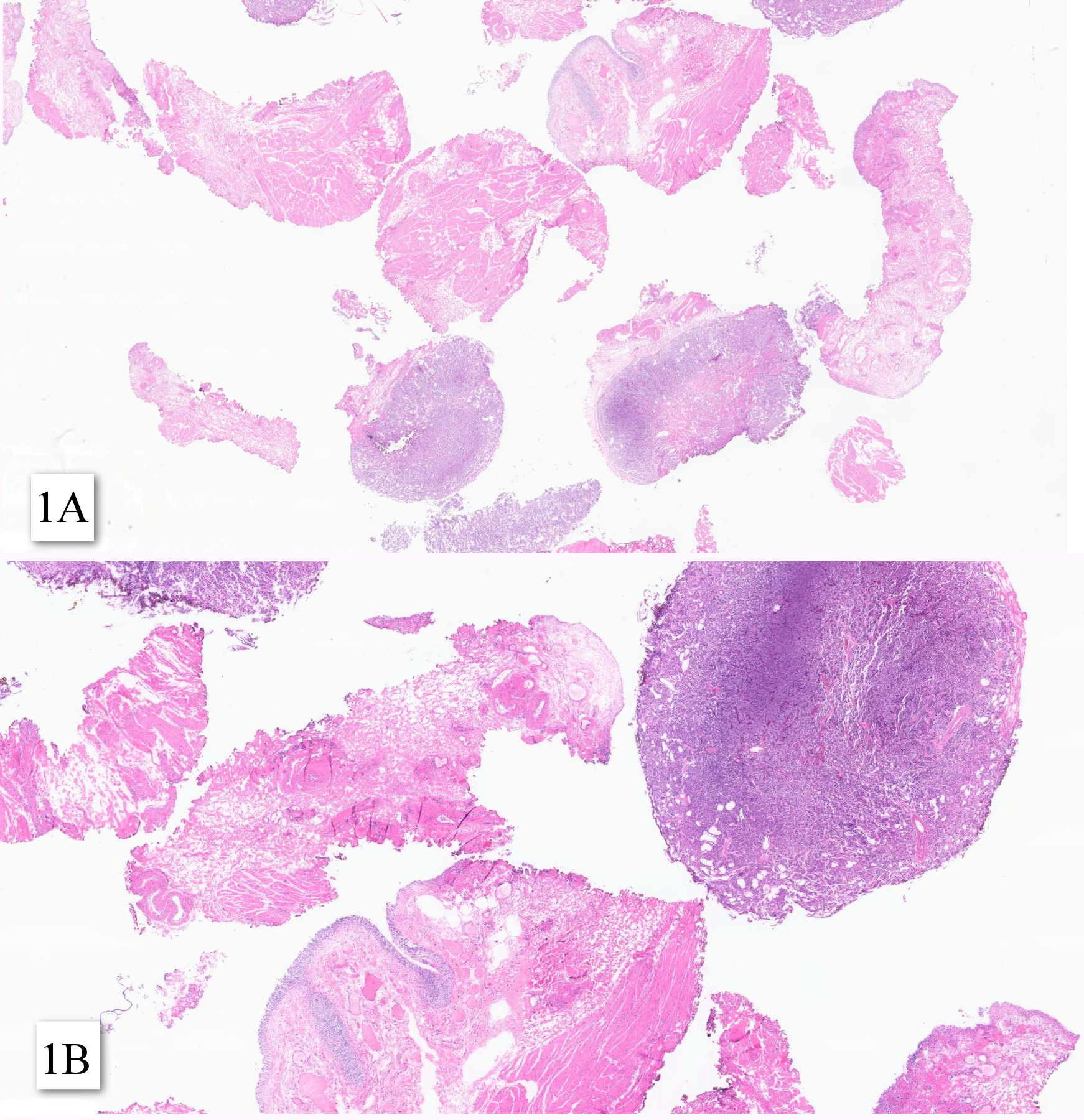
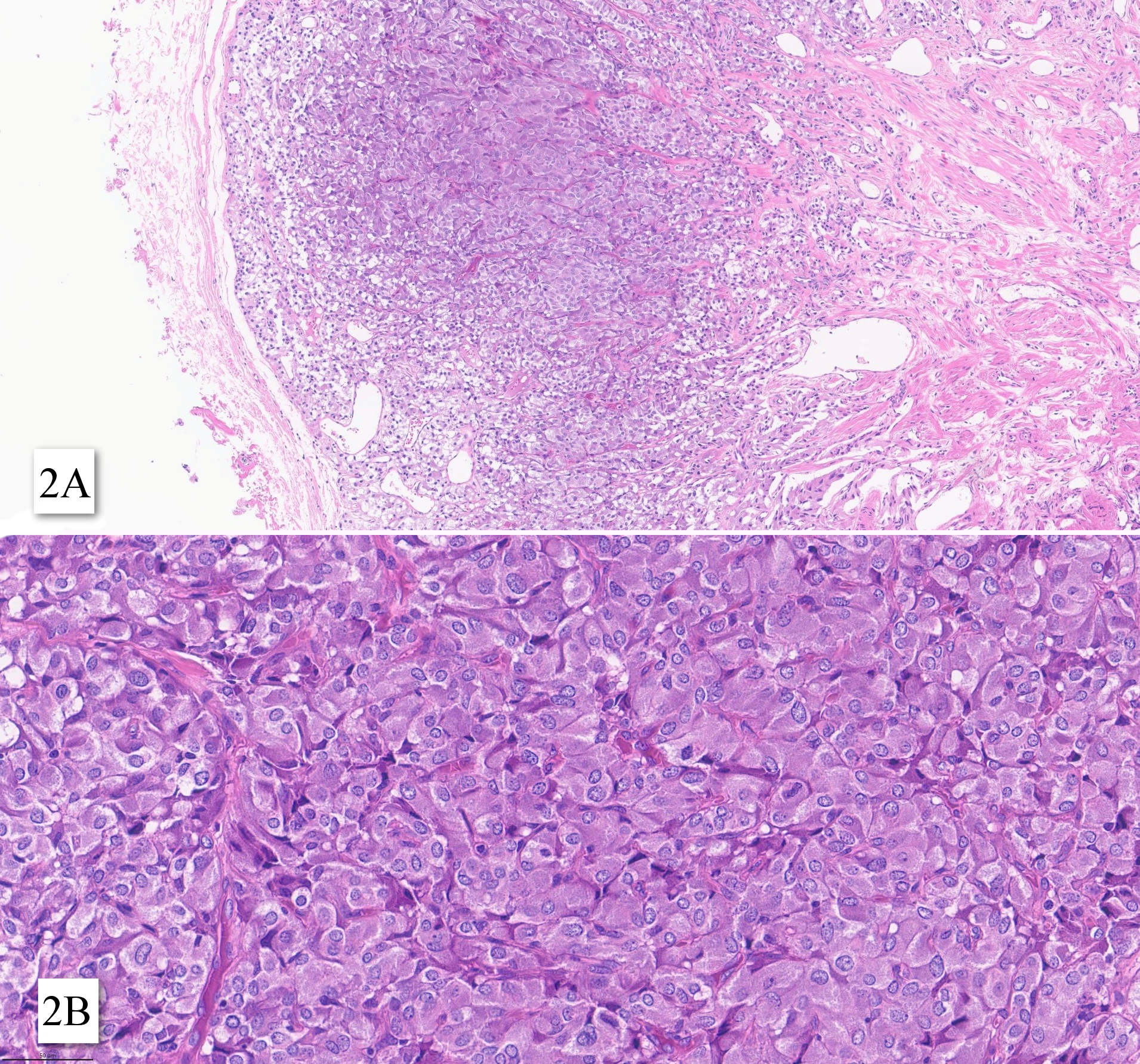
A female patient in her late 60s underwent surgical removal of bladder tumor. The first pathology report had the diagnosis of poorly differentiated carcinoma.
Contributors :
Vinicius Barros Figueiredo
Oncoclinicas Precision Medicine
Belo Horizonte, Minas Gerais, Brazil
Daniel Athanazio
Oncoclinicas Precision Medicine
Federal University of Bahia
Salvador, Bahia, Brazil