CASE OF THE MONTH
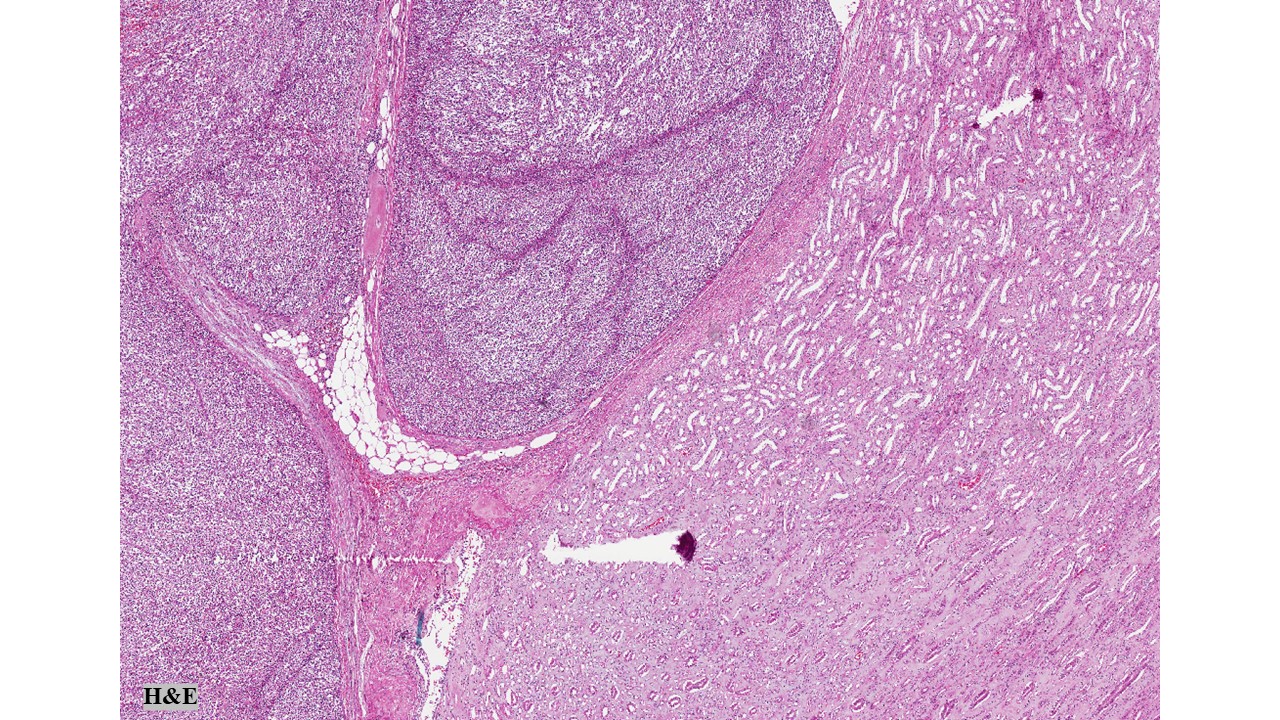
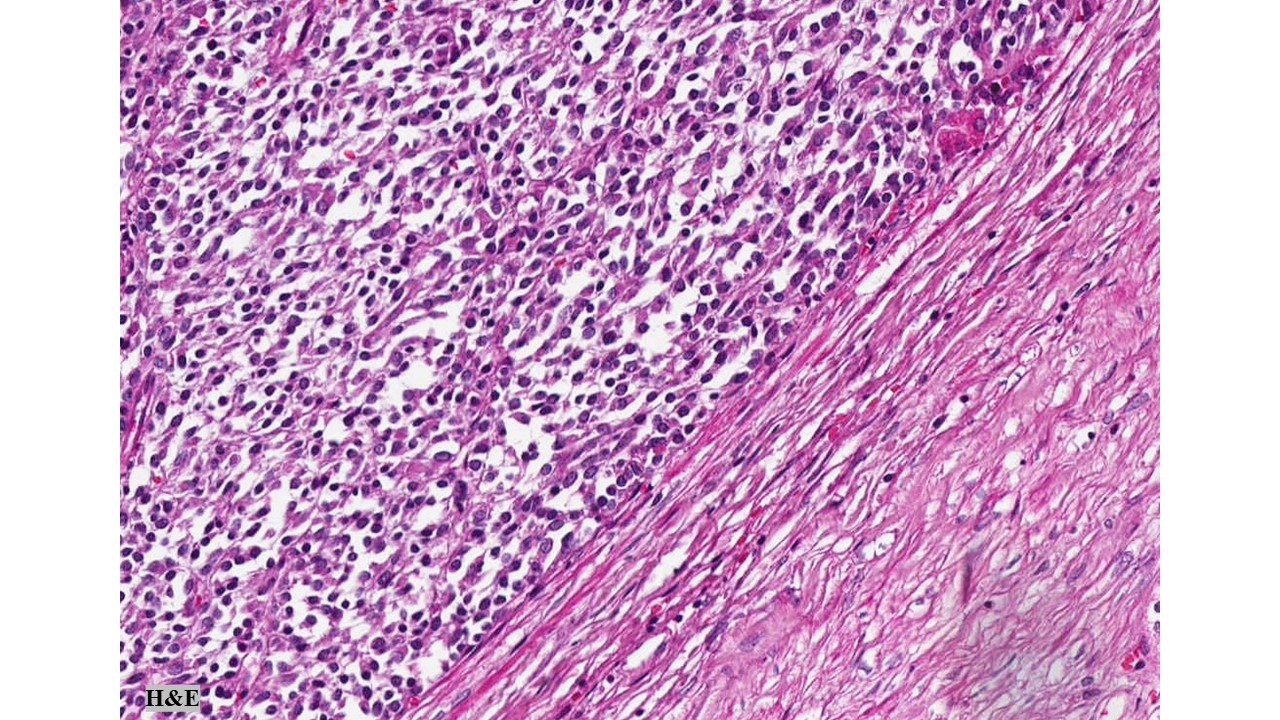
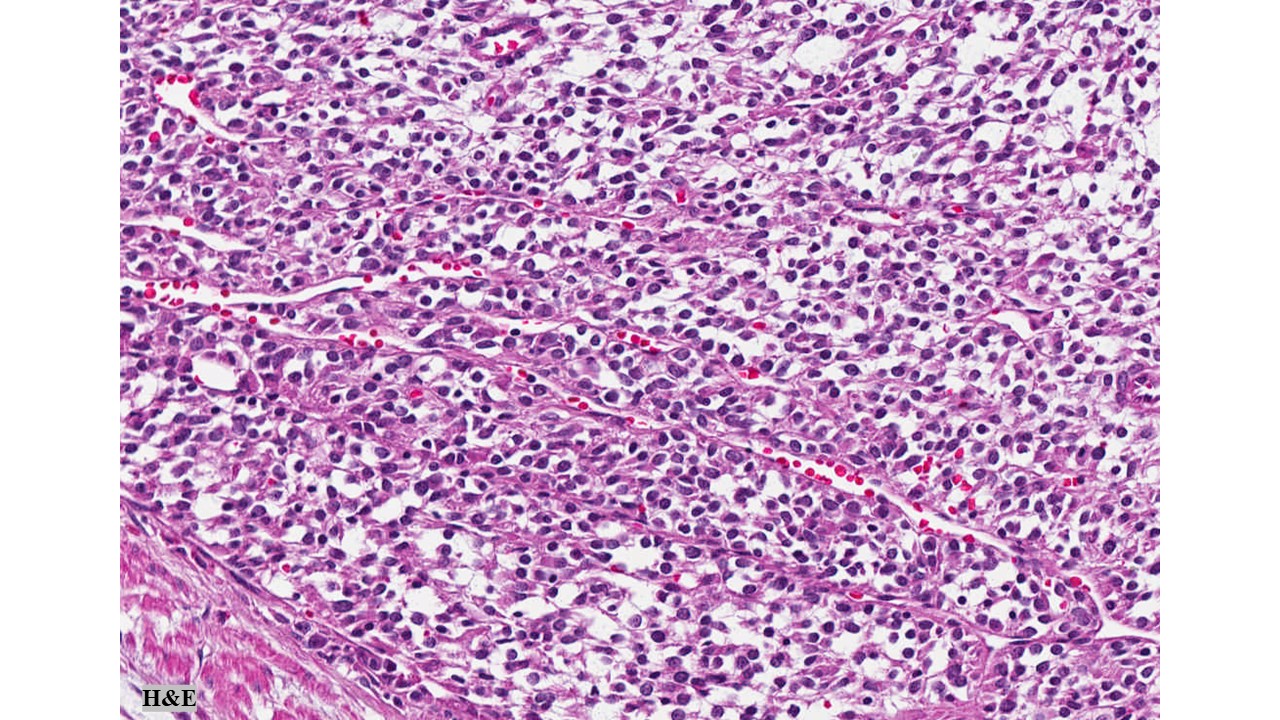
A 38-year-old male presented with a history of persisting right flank pain. Ultrasonography revealed a 10 cm mass in the mid-portion of the right kidney at the corticomedullary junction. A CT-guided biopsy revealed a spindle cell neoplasm of uncertain malignancy. The patient underwent a right nephrectomy, which revealed a 10×6×5 cm solid tumor with vascular invasion. On gross examination, the tumor was grayish white with areas of hemorrhage and necrosis.
Contributors :
Ekta Jain, MD, PostDoctoral Clinical Research Fellow, The University of Alabama at Birmingham, Alabama
Rodolfo Monitorini, MD, IFCAP, Molecular Medicine and Cell Therapy Foundation, Università Politecnica delle Marche, Ancona, Italy
Cristina Magi-Galluzzi, MD, PhD, FCAP, Professor & Chair of Pathology, The University of Alabama at Birmingham, Alabama