CASE OF THE MONTH
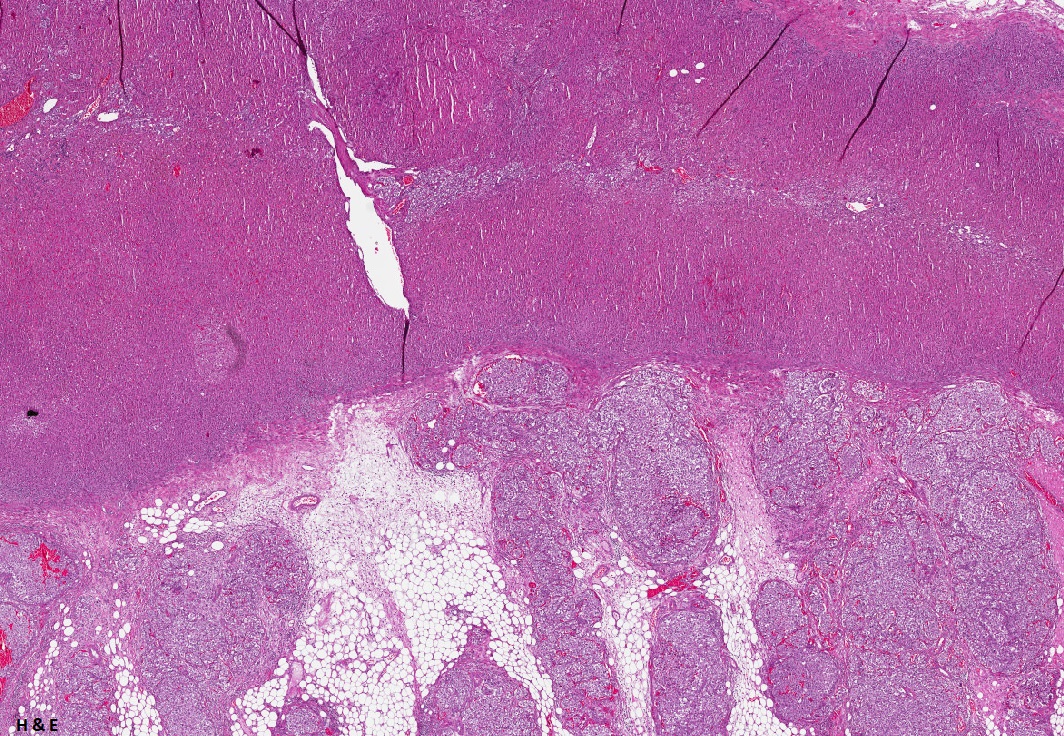
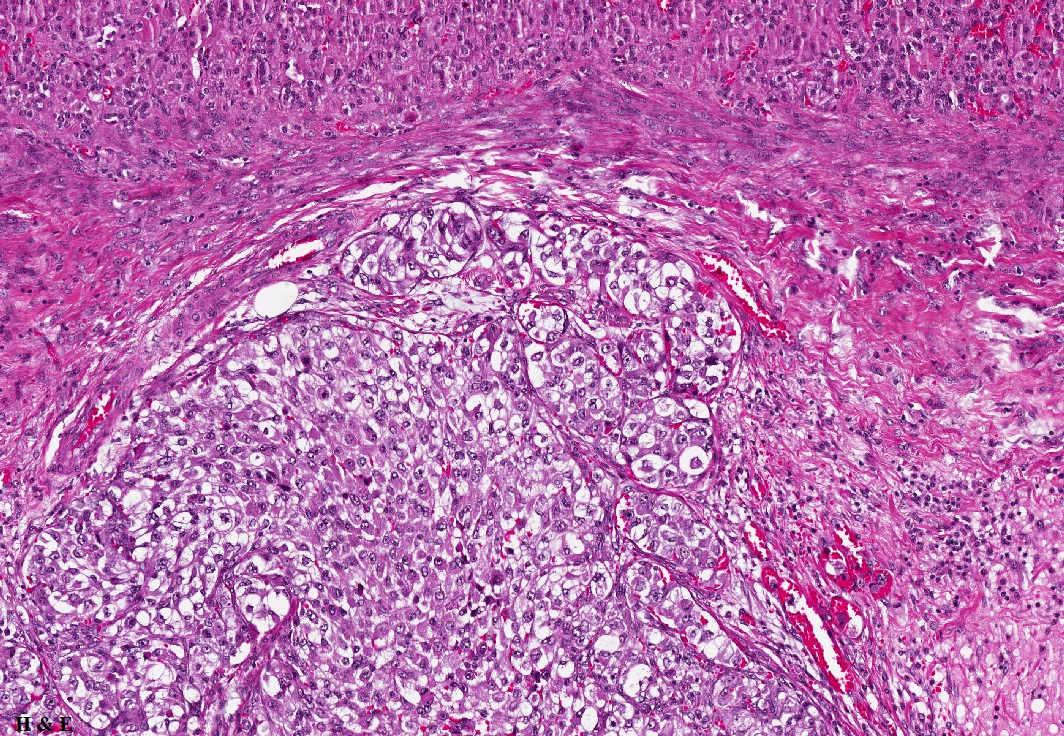
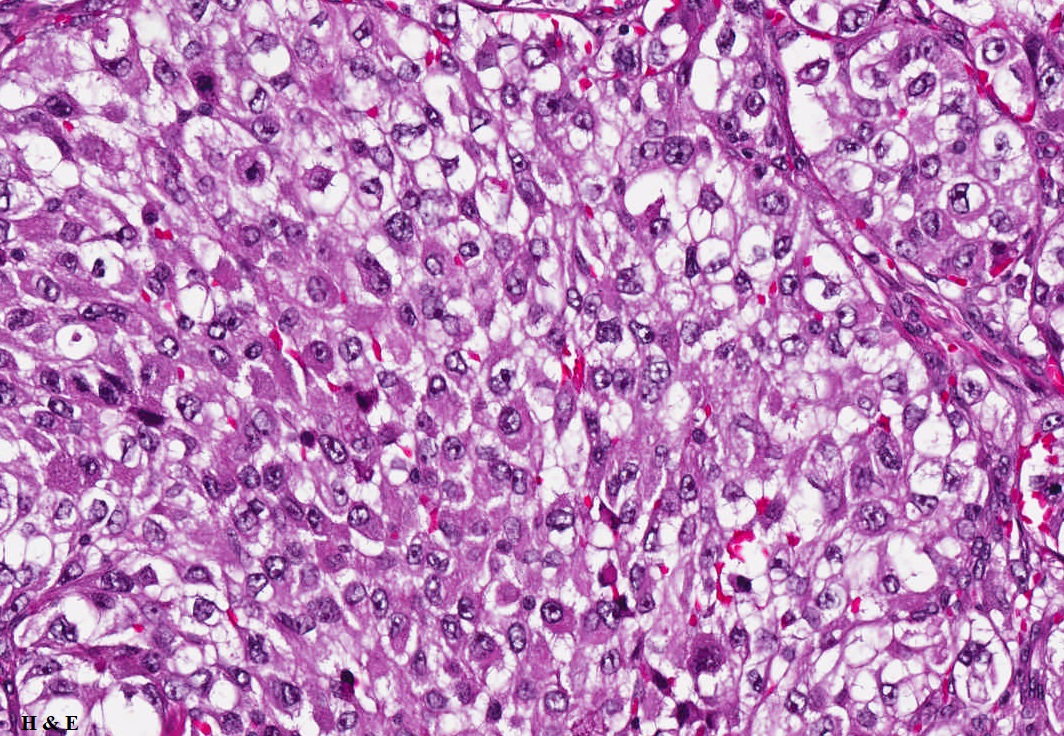
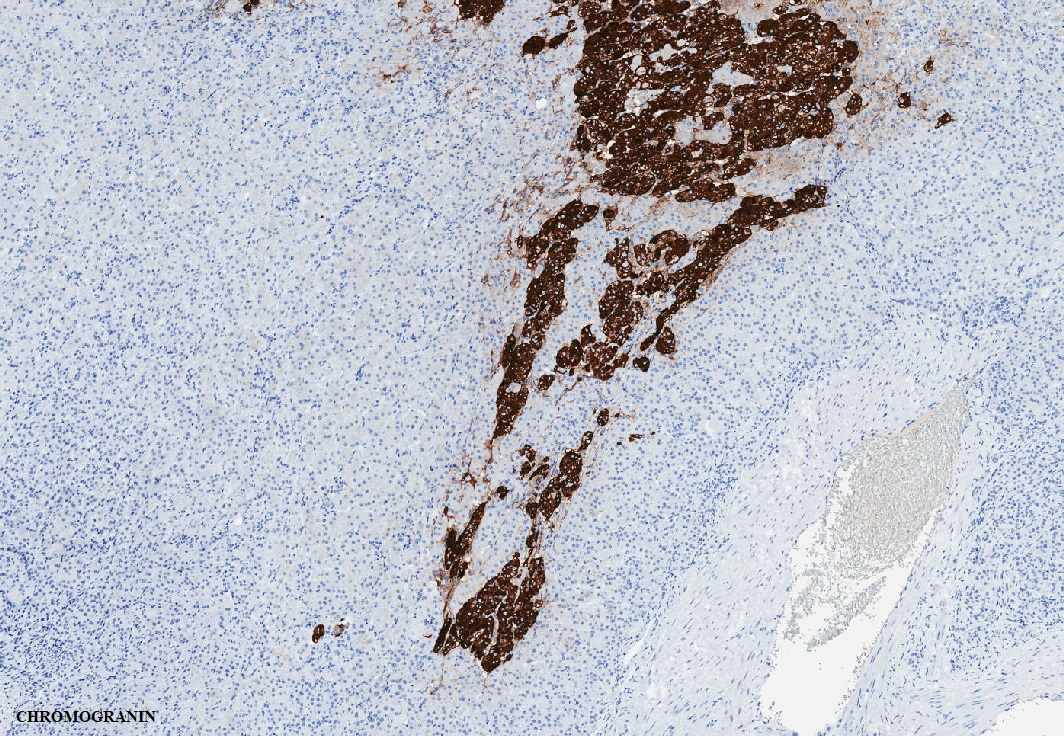
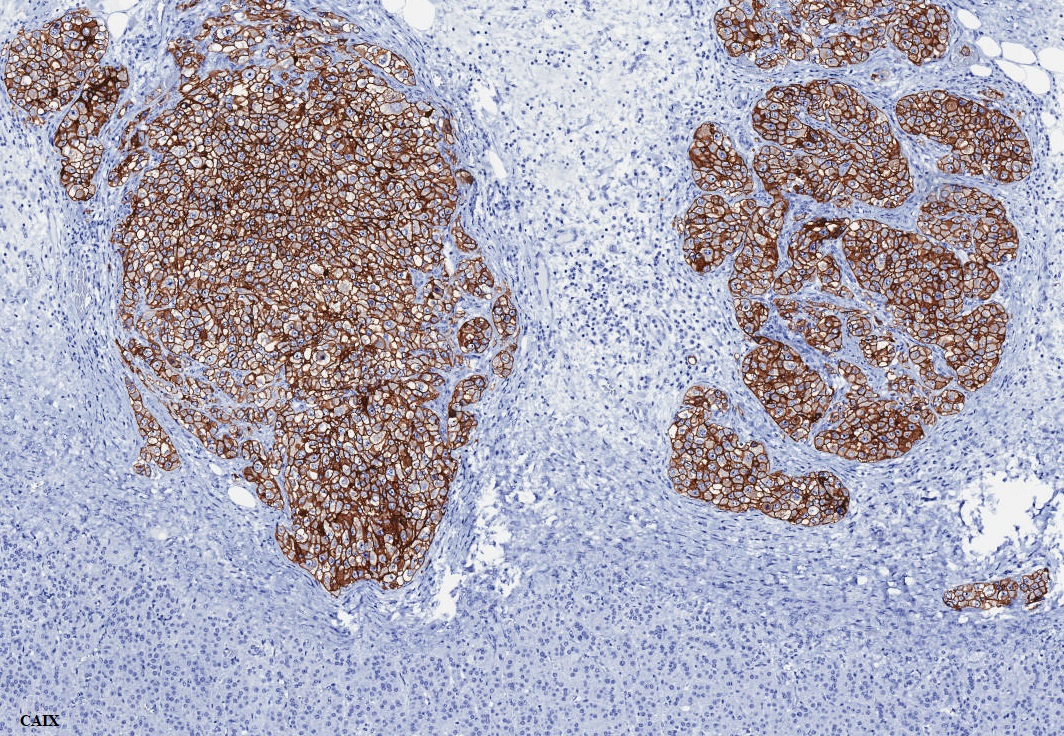
A 65-year-old man presents with a 5 cm mass in the left adrenal gland. He has a prior history of a renal cell tumor (though specific details are not available)
Contributors :
Ekta Jain, MD, PostDoctoral Clinical Research Fellow, The University of Alabama at Birmingham, Alabama, USA
Rodolfo Monitorini, MD, IFCAP, Molecular Medicine and Cell Therapy Foundation, Università Politecnica delle Marche, Ancona, Italy
Cristina Magi-Galluzzi, MD, PhD, FCAP, Professor & Chair of Pathology, The University of Alabama at Birmingham, Alabama, USA