CASE OF THE MONTH
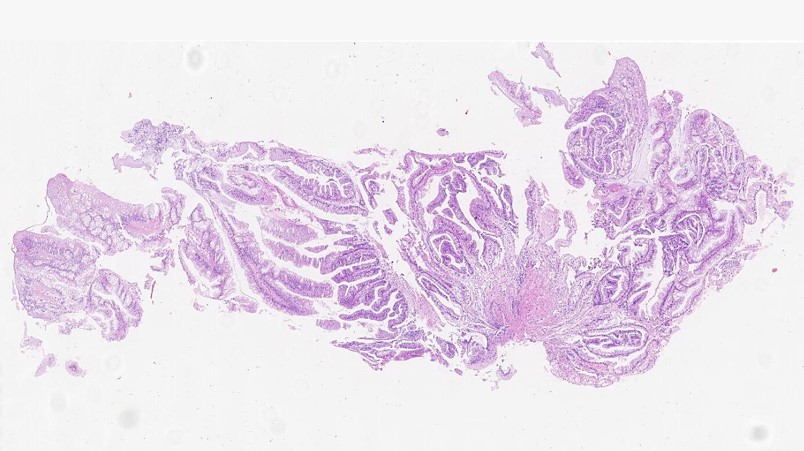
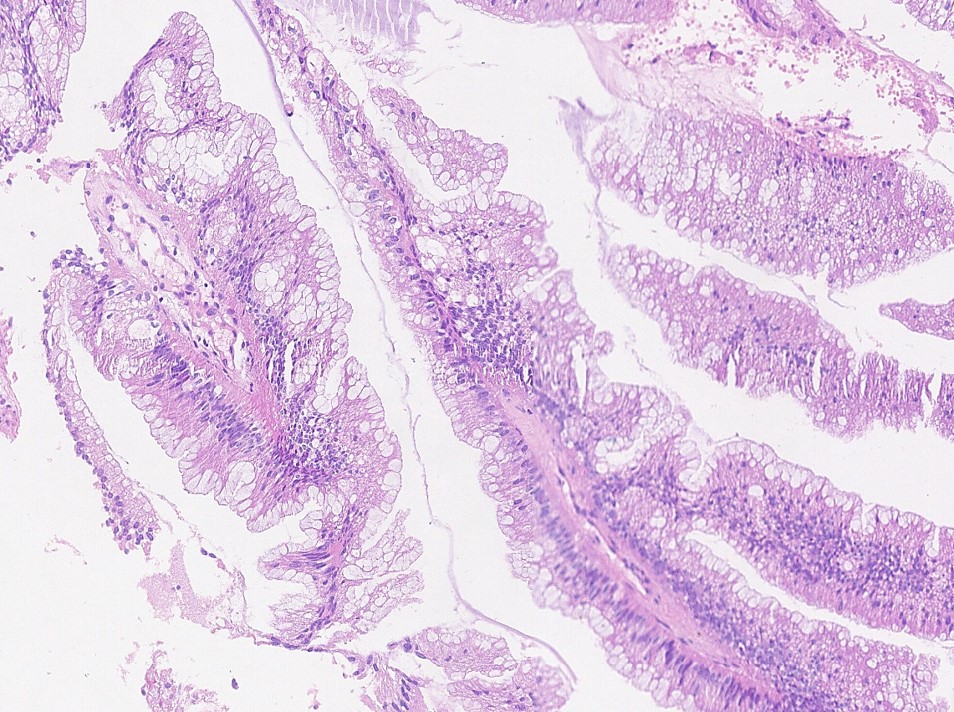
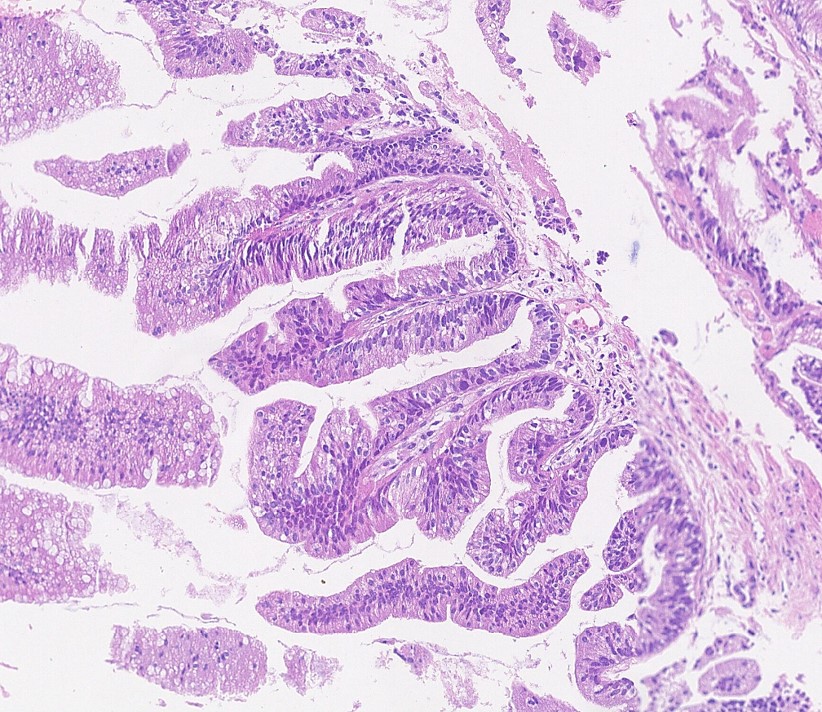
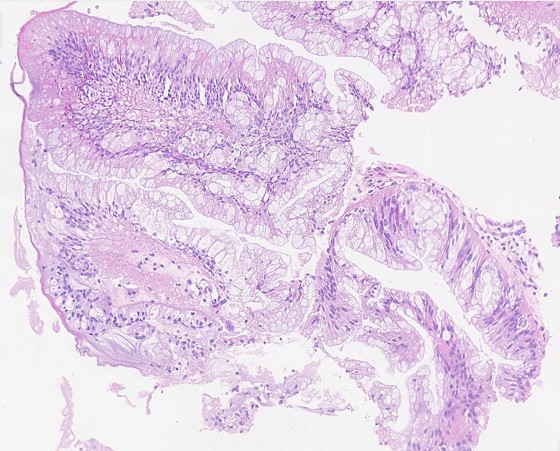
A female patient in her 80s underwent surgical removal a bladder lesion.
Contributors :
Maiara Ferreira de Souza
Oncoclinicas Precision Medicine
Recife, Pernambuco, Brazil
Luiza Barbosa Oliveira
Oncoclinicas Precision Medicine
Salvador, Bahia, Brazil
Daniel Athanazio
Oncoclinicas Precision Medicine
Federal University of Bahia
Salvador, Bahia, Brazil